 Call 020 8502 1777 or
Call 020 8502 1777 or  online form
online form- March 2016 (1)
- November 2015 (1)
- February 2015 (1)
- January 2015 (1)
- July 2014 (2)
- June 2014 (1)
- May 2014 (1)
- April 2014 (2)
Preparing for the London Marathon
Premier Podiatry’s Sports Scientist, Ken Hoye reflects on our experience in the build up to the London Marathon.

It’s that time of year again.
The time when we see many runners old and new heading out on the streets to begin their marathon training. London, Brighton, maybe a marathon overseas, all suggest marathon training should be under way. You could be one of those who are already well in to laying the foundations, or one who is yet to muster a steady run but by now you will be getting ready for the big push towards long Sunday runs, midweek tempo’s and some recovery runs to add up the miles.
At Premier Podiatry some of us are marathon training (although not quite as far along as we would have liked, but plenty of time yet hey?) and some of us are not, but for us “this” time of year is the time when we begin to see the first overuse injuries of the spring. Runners suffer many kinds of injuries (up to 80% of runner will get an injury in a given year) but “overuse injuries” are the most common. I could argue with this title as it is possibly not scientifically correct but let’s go with it for the time being.
In the case of marathon runners the main reason we get these kinds of issues is that we run. One foot in front of the other, up to 1500 times a mile, for mile after mile. A repetitive action can bring about repetitive strain issues. Sometimes we cross train, sometimes we lift weights, some runners even do Pilates or yoga (yes really) but most only ever do these things when they cannot run. How many people would write “Gym session” in the diary when they could write “miles”? Not as many as really should. I know intelligent and sensible people who think it’s a good idea to go from little or no running to 50 or more miles per week and throw in a speed session or two just for good measure.
The problem with many of the injuries ‘caused’ by marathon training is that they often have a long lead time when the stress builds up but you have no symptoms, then in a case of “the straw that breaks the camel’s back”, any given run can initiate pain. The other and bigger problem with this is that as these issues take a while to build up, they often also take a while to recover from. As any marathon runner will know, time is our main adversary, in every training run (to a greater or lesser extent), in days until the start (105 for me and counting….), and on the day itself where hours and minutes tick past far too quickly.
So what injuries? ITB syndrome, calf and Achilles pain, shin pain issues (amongst others) are all common this time of year and their frequency will increase rapidly until March or April when they will begin to reduce almost as fast. All of these can be treated, although some quicker than others but many will make the start line having come through our door seeking help. But many others will not make it, either through unfortunate timing, seeking help too late or by not rehabbing properly.
The other over riding thing about these kinds of injuries are that most are preventable. Today more so than ever before, we can find the problems before they begin, or at least before they really become a threat to that marathon PB or finishers medal.
For us the most obvious way is to use our 3D gait technology. The system uses infra-red cameras and silver markers (think animation for films and video games) to compare your running style (Gait) with the largest data base around, to help us find any imbalances that could become these injuries.
The weakest links in the chain can be identified and addressed before you push them past their limits. In short we could prevent the injury that could stop you from making the start line. In many cases we could improve your performance too.
So whilst we will be happy to see you in March or April and we will do our best to get you to the start line, why not make life easier and let us help you rewrite your personal best this spring.
Ken Hoye
To enter our marathon competition, click here.
For more information on gait analysis and to download our free brochure click here
If you would like more information or have a question, please contact us.
Gait analysis of an elite runner

“The 3D gait analysis is an incredibly useful exercise, and has helped to flag up issues with the way I move that might eventually lead to injury. To maintain consistent training it’s really important to avoid problems before they arise. I hope this session should hopefully help me avoid time on the physio’s couch in the future!
The guys have also pinpointed a few areas to for me to work on which should help improve performance. I would highly recommend this to other runners who are looking to knock some time off their PB’s.”
Shaun Dixon
UK Fell Running Champion
Barefoot running – the debate rages on
Although there has been a drop off in the number of runners using the barefoot approach, the lack of evidence either way in this field means the debate will continue. The recent publication of the results of an online survey has re-ignited this debate with analysis and subsequent comments on the excellent blog produced by Craig Payne (http://www.runresearchjunkie.com/barefoot-running-survey-evidence-from-the-field/).
In my opinion, the type of shoe required is in part determined by the underlying structure but, as importantly, the interaction of the whole lower limb / pelvis. Someone with a mildly pronated foot type may pronate more due to poor overall limb control and benefit from a shoe with stability. However, this is addressing the symptom not the cause. Improve the function and you may reduce the need for stability. By contrast, someone with a significantly pronated foot type is likely to require more support. Transitioning to a different foot strike pattern has the dual possibility of either reducing or increasing injury risk / rate.
The example gait below shows a physical fitness trainer who is very keen on the barefoot approach for himself. The ankle results show a reduced degree of peak pronation and slightly increased time to peak pronation as would be expected with a forefoot strike. However, you will note that the asymmetry present in a neutral shoe with 8mm drop is still present barefoot and, if anything, is worse in terms of tibial rotation. Thus we can change things by going to barefoot but not necessarily improve function.
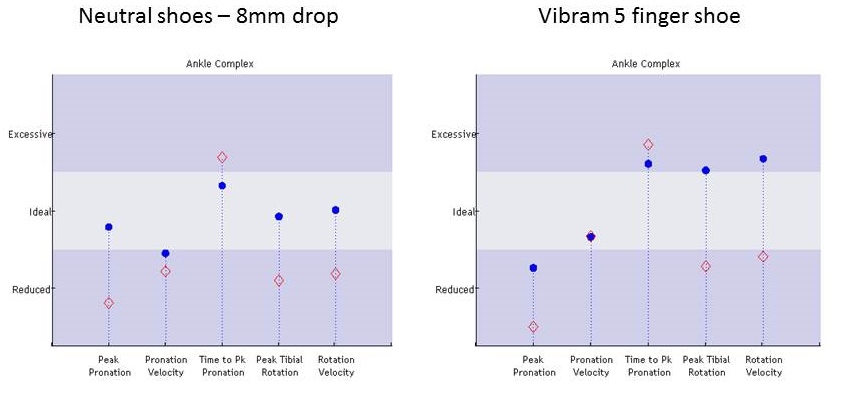
Barefoot running, as expected, reduces peak pronation and time to peak pronation but does not resolve the asymmetry which, if anything, gets worse in terms of tibial rotation. Click on picture for enlarged copy.
More importantly the hip / pelvic values clearly show that the altered demands of barefoot running require greater hip control which he clearly does not have. One can only assume this places him at more risk. So, in his instance, a more traditional running pattern / shoe may be a better option unless he addresses the muscle imbalance to allow the altered running style. However, he may be able to keep with this dysfunction to a certain level of activity. Past this level and with increasing fatigue, the risk of injury increases. This can be moderated by a structured approach to increasing activity levels (i.e. a graduated load response) but, intuitively, there will be a maximum threshold after which injury is more likely. Of course we also need to consider all the extrinsic factors such as running surface etc.
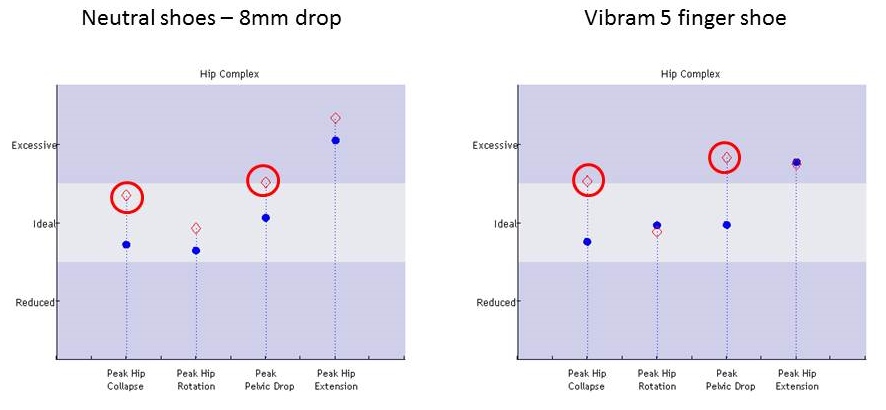
At the hip, rotation and pelvic drop are worse barefoot. Click on picture for enlarged copy.
Thus which shoe and which style an individual utilises will depend on their overall function both structurally and dynamically. My current approach with patents is to optimise function as much as possible with structured rehabilitation programmes and then determine the level of support or gait modifications that may be required to minimise injury. If they are unable or not prepared to do the necessary work to achieve this then they have to accept that their function is a compromise and they may not be able to exercise to their desired level without injury. However, we hope that we can at least educate in this regard and thus allow them to make an informed decision in terms of training and exercise levels.
It is less about extremes and more about a balanced approach, optimising function and then managing around individual limitations. Therein lays the skill as one size does not fit all.